

PEPTIC ULCER DISEASE.
It is a major gastro-intestinal disease, which is common among the majority of the populace. Normally, we have the stomach lining subdivided into the pre-epithelial, epithelial and the sub epithelial.
The pre-epithelial consist of the mucus, bicarbonate and phospholipids; the epithelial is responsible for cellular resistance, cell proliferation and restitution, while the sub epithelial is responsible for blood flow.
The pre-epithelial consist of the mucus, bicarbonate and phospholipids; the epithelial is responsible for cellular resistance, cell proliferation and restitution, while the sub epithelial is responsible for blood flow.
The alkaline rich mucus that is found at the pre-epithelium protects the stomach and duodenum from the drastic effect of acid. But, these mucosal cells that help in the secretion of mucous can be damaged by bacteria /viral infection, certain drugs such as nonsteroidal anti-inflammatory drugs e.g. aspirin.

When these mucosal cells are damaged there will be reduced alkaline rich mucous hence the gastric acid secreted by lumen can pass through the pre-epithelium then into the epithelium causing injury/wound on the epithelium of the stomach, this is known as peptic ulcer disease.
Peptic ulcer disease can be divided in two major part which are, gastric ulcers and duodenal ulcers.

GASTRIC ULCERS.
They are associated with stress, NSAIDs or bacteria, gastric ulcer is manifested by painless bleeding which takes longer time to heal thus, and gastric ulcers are chronic. Other risk factors of gastric ulcers are cigarette smoking, excessive alcohol intake, caffeine and also fatty food.
HOW THE BACTERIUM (H.PYLORI) CAUSES ULCER.
It secretes some cytotoxins that cause inflammatory processes thus leading to PUD. It also secretes enzymes that can cause tissue damage e.g. urease, neuramidase etc.
NON STEROIDAL ANTIINFLAMMATORY DRUGS.
They inhibit cyclo oxygenase which is a precursor for the biosynthesis of prostaglandins using arachnoid acid thus leading to reduced production of prostaglandin which provides protective covering to the epithelium of the stomach.
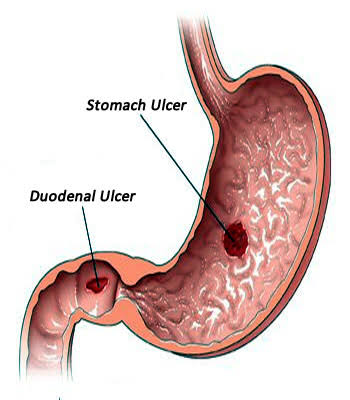
DUODENAL ULCERS.
They occur at any age, occur both in men and women and its manifested by abdominal pain, its associated with cigarette smoking, NSAIDs and H.pylori
Also, PUD can be classified into benign and malignant PUD. In benign, there is normal gastric acid production but the mucosal barrier is weak while for malignant; there is excessive secretion of gastric acid that overwhelms the mucosal barrier.
GENERAL SIGNS AND SYMPTOMS OF PEPTIC ULCER DISEASE.
Epigastric pain (pain in the upper part of the abdomen, it occurs 1-3 hours after meal.
Anorexia
Weight loss
Nausea
Vomiting
Haemorrhage
Chronic iron deficiency anaemia
Pyloric stenosis.
ALARM FEATURES OF PEPTIC ULCER
DISEASE.
Dysphagia.
Unintentional weight loss.
Gastrointestinal bleeding.
Persistent vomiting.
METHOD OF DIAGNOSIS OF PEPTIC ULCER DISEASE.
Endoscopy.
Radiology.
Serological examination.

ENDOSCOPY.
Here an anaesthetics is given, then a lighted thin tube attached with a tiny camera is passed through the throat and into the stomach then to the duodenum. This allows the physician to access the lining of the GI tract to detect ulcers.

RADIOLOGY.
This is done to evaluate a patient to know if the patient’s present symptoms are that of peptic ulcer disease. Barium meal is administered, after which x-ray is done.

SEROLOGICAL EXAMINATION.
This is done to detect the present of H. pylori in the G.I.T. it is not a real test to diagnose peptic ulcer disease per say, it is just to know if H. pylori is implicated or not, because if yes, it will affect the treatment approach.
CLASSES OF DRUGS USED IN PEPTIC ULCER DISEASE.
Antacids.
H2 Receptor Blockers.
Mucosal Protective Agents.
Proton Pump Inhibitors.
Anticholinergics.
Prostaglandin Analogs.
Anti-microbial Agents.

ANTACIDS.
These are alkaline substances that neutralize acids e.g. aluminium, magnesium, and calcium compounds.
They enhance the secretion of mucus, bicarbonate and prostaglandins. They have a quick onset of relief but last for a short duration. They exist in different forms which includes carbonate, hydroxide, oxide and trisilicate.
They can also be used to relieve painful symptoms associated with gas (antiflatulence). They only provide relieve of pains.
SIDE EFFECTS OF ANTACIDS.
Aluminium and calcium: constipation.
Magnesium: diarrheal.
Calcium carbonate: produces gas and bleeding, therefore, often combined with simethicone. Excess use of calcium antacid can cause kidney stones and rebound hyperacidity.
DRUG INTERACTIONS.
Concurrent use of other drugs with antacids causes decrease in the absorption of the other drug into the systemic circulation, it may chelate with some drugs leading to inactivation of the other drug, and produces insoluble complexes thus reduced drug absorption.
CAUTIONS IN THE USE OF ANTACIDS.
Antacids are contraindicated in fluid imbalances, renal diseases, heart failure, pregnancy and G.I obstruction.
Patients with hypertension should use low sodium antacids such as Maalox.
Most medications should be given 1 to 2 hours after giving antacids.
Concurrent administration of enteric coated medications with antacids should be avoided.
Monitor for side effect such as nausea, vomiting, abdominal pain, diarrheal, constipation and acid rebound Monitor for therapeutic response.
Caffeine, alcohol, harsh spices and black pepper may aggravate the underlying GI condition, thus, should be avoided.

HISTAMINE 2 RECEPTOR BLOCKERS.
Normally, histamine 2 stimulates the secretion of acid by the parietal cells. Histamine 2 blockers antagonizes the H2 receptors hence causes decrease in hydrochloric acid secretion.e.g. cimetidine, ranitidine.
H2 blockers reduce hydrogen ion secretion from the parietal cells which results in an increase in pH of the stomach giving the patient relief from symptom.
The dosage should be reduced in pregnancy. Cimetidine affects the cytochrome p450 metabolising system in the liver, it may also cause confusion and antiandrogenic effects (gynecomastia).
Ranitidine is more powerful, it is used for up to 8 weeks. Antacids may be given concurrently to relief pain.

PROTON PUMP INHIBITORS.
These are strong inhibitors of gastric acid secretion, they bind irreversibly to the gastric proton pump to prevent the release of gastric acid from parietal cells.e.g. Omeprazole, esomeprazole, rabeprazol, lansoprazole, pantoprazole.
They inhibit H+-k+-ATPase hence reducing hydrogen secretion. They are more effective than H2 receptor blockers, they produce faster relief of symptoms and faster healing, used in the treatment of H.pylori associated ulcers.
Side effects are nausea, diarrheal, may increase serum levels of diazepam, phenytoin and cause increased chance of bleeding when used with warfarin.
PROSTAGALNDIN ANALOGUE.
Example is misoprostol, it is the synthetic form of prostaglandin E, it has a cytoprotective activity, it protects the mucosa from injury by enhancing local production of mucous or bicarbonate, it also helps to maintain mucosal blood flow. Indicated for patients at high risk of GI ulceration and bleeding and in those who take NSAIDs.
It is contraindicated in women of child bearing age and during pregnancy cause it may induce abortion and teratogenesis.
Side effects are diarrheal and abdominal cramps.

ANTICHOLINERGICS.
Example is pirenzepine, it is a muscarinic M1 acetylcholine receptor antagonist, it blocks acid secretions but it is rarely used instead used as an adjunct therapy. Side effects include; anorexia, blurred vision, constipation, dry mouth, sedation.
MUCOSAL PROTECTIVE DRUGS.
Examples are chelated bismuth, sucralfate
Chelated bismuth protects the ulcer crater and allows healing, it has some activities against H. pylori, should not be used repeatedly or for more than 2 months at a time, can cause black stools, constipation.
Sucralfate is the preparation of sulphated sucrose and aluminium hydroxide that binds to the normal and ulcerated mucosa. It binds to the ulcer and form a protective barrier between the mucosa and gastric acid, pepsin and bile salts and also stimulates prostaglandin’s synthesis.
Side effects include constipation and dry mouth. It cannot be given with antacids, H2 receptor blockers, proton pump inhibitor, may bind with other drugs to prevent their absorption, therefore, give 2 hours after other drugs.
SPECIFIC TREATMENT APPROACH.
H. pylori associated; here, either conventional ulcer drugs or the use of antibiotics can be adopted.
CONVENTIONAL APPROACH.
First combination; omeprazole 20mg, clarithromycin 500mg and Amoxicillin 1g.
Second combination; Omeprazole 20mg, Clarithromycin 250mg and metronidazole 400mg (This is a fixed dose combination administered for a period of one week).
H. pylori is resistant to metronidazole, hence, necessitating the need to replace metronidazole.
Third combination; bismuth salicylate, metronidazole, amoxicillin or tetracycline and proton pump inhibitor.
NSAIDs associated ulcers; first and foremost discontinue the use of NSAIDs, if the peptic ulcer disease is not resolved then standard doses of proton pump inhibitors, H2 blockers, misoprostol, antacids and sucralfate can be used.
The best to be used in the management of NSAIDs induced peptic ulcer disease is proton pump inhibitor because they have the fastest therapeutic outcome. It has a rapid killing ulcer rate.
Here the following can be employed;
Omeprazole 200mg bd or 400mg od is being administered for a period of 8 weeks. For omeprazole administered 200mg for 8 weeks 80% therapeutic outcome is achieved, for omeprazole administered 400mg for 8 weeks 79% success is achieved.
Therefore, it is better to administer omeprazole in a divided dose than in a single/daily dose regimen. Alternatively, ranitidine can be administered in a dose strength of 150mg bd or 300 od for a period of 8 weeks but 63% success is achieved.
But if it necessary that a patient should take NSAIDs then the drugs listed above should be taken in combination with proton pump inhibitor or misoprostol.
NON PHARMACOLOGICAL APPROACH.
Lifestyle modification; reduce alcohol intake, cigarette cessation, weight loss, physical activity, diet modification e.g. reduce fatty food content, reduce caffeine intake, reduce chocolate intake.
Check the drug history of the patient.
Top Post People are reading.
1. (10) WordPress Plugins for SEO.
2. How to Rank higher on Google.
3. Football betting tips, 100% sure.
4. African Fish Roll Preparation.
5. 10Fastest way to make Money with a Blog.
6. How to create smiley and icon.
7. How to send free SmS by Gmail.
8. Hustler Tools and Tips.
9. Promote yourself or business on Sharpest Arena.
10. How to Create a Blog.
11. How to Submit Sitemap to search engine, using webmasters.
12. 11Useful WhatsApp Tricks.











{kind=link}
{kind=link}
{kind=link}
0 Comments